

Dr. Marco V. Benavides Sánchez. Medmultilingua.com /
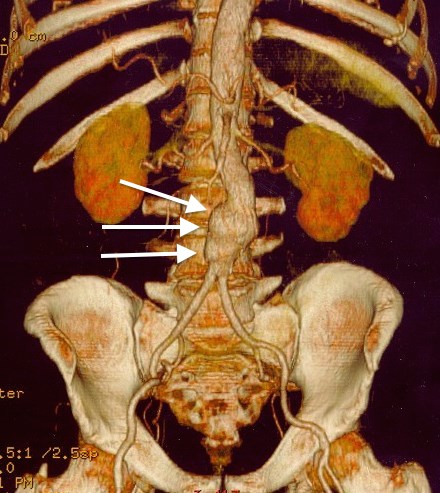
Abdominal aortic aneurysms (AAA) are one of medicine’s quietest dangers. They grow slowly, often without symptoms, deep within the body’s largest artery. And when they rupture, the consequences are catastrophic. For decades, doctors have relied on a simple rule of thumb to decide when to intervene: measure the aneurysm’s diameter, and if it crosses a certain threshold, consider surgery. It’s a guideline that has saved countless lives, but also one that leaves many questions unanswered.

Now, a new wave of artificial intelligence is beginning to challenge that long‑standing paradigm. Instead of treating every aneurysm as a uniform balloon waiting to burst, researchers are teaching AI systems to read the subtle geometry of each patient’s arterial wall—its curves, its stresses, its unique patterns of growth. The goal is ambitious: to predict how an individual aneurysm will evolve, long before it becomes dangerous.
A recent commentary by Antonio Bozzani, Pietro Cerveri, Vittorio Arici, and Giulia Maria Stella highlights just how transformative this shift could be. Their analysis, published in Artificial Intelligence in Medicine, reflects on emerging research that uses geometric deep learning—a branch of AI designed to understand complex shapes—to forecast local growth on the surface of aneurysms. It’s a technique that moves beyond simple measurements and into the realm of personalized risk.
At its core, geometric deep learning allows computers to interpret the body not as a flat image, but as a three‑dimensional landscape. Imagine the aneurysm’s surface as a rugged terrain, with peaks and valleys that reveal where the arterial wall is stretching or weakening. Traditional imaging can capture this terrain, but AI can analyze it with a level of detail no human eye could match. By learning from thousands of examples, these models begin to recognize patterns—areas that tend to expand faster, regions under mechanical stress, and subtle warning signs that might predict future instability.
For patients, this could mean a future where decisions about surgery are no longer based solely on size, but on a personalized map of risk. Two aneurysms of identical diameter might behave very differently, and AI could help clinicians distinguish between those that are quietly stable and those that are silently accelerating toward danger.
But the authors of the commentary are careful to emphasize that this technological leap must be grounded in clinical reality. AI, they argue, should complement—not replace—established medical guidelines. The promise of precision medicine is powerful, but it must be balanced with transparency, rigorous validation, and interpretability. In other words, doctors need to understand not just what the AI predicts, but why.
This is especially important in a field where decisions carry profound consequences. Operating too early exposes patients to unnecessary risks; waiting too long can be fatal. The integration of AI into this delicate decision‑making process requires trust, and trust must be earned through evidence.
That evidence is beginning to accumulate. Early studies show that geometric deep learning models can identify growth hotspots with surprising accuracy. Some can even simulate how an aneurysm might change over time, offering a glimpse into the future of a patient’s vascular health. Yet these models must be tested across diverse populations, imaging technologies, and clinical settings before they can be widely adopted.
The commentary also touches on a broader theme: the evolution of medical guidelines themselves. Historically, guidelines have been shaped by large clinical trials and population‑level data. But as AI enables more individualized predictions, the authors suggest that guidelines may need to adapt. Instead of rigid thresholds, future recommendations might incorporate dynamic, data‑driven assessments tailored to each patient’s anatomy and risk profile.
{kind=link}
This shift mirrors a larger transformation happening across medicine. From oncology to cardiology, AI is helping clinicians move away from one‑size‑fits‑all approaches and toward precision strategies that reflect the complexity of human biology. The challenge is ensuring that these tools enhance clinical judgment rather than overshadow it.
For patients living with an abdominal aortic aneurysm, the implications are profound. Instead of waiting anxiously for a number on a scan to cross an arbitrary line, they may one day receive a detailed, personalized forecast of their condition—one that empowers them and their physicians to make informed, timely decisions.
The authors’ message is ultimately one of balance and optimism. Artificial intelligence, when used responsibly, can illuminate aspects of disease that were once invisible. It can help clinicians see not just what is happening inside the body, but what might happen next. And in the case of aneurysms—silent, unpredictable, and often deadly—that foresight could save lives.
As AI continues to weave itself into the fabric of modern medicine, the story of aneurysm prediction offers a glimpse of what’s possible when technology and clinical wisdom evolve together. It is a reminder that innovation is most powerful when it respects the foundations on which it stands.
Reference
Bozzani, A., Cerveri, P., Arici, V., & Stella, G. M. (2026). Comment on: “Geometric deep learning for local growth prediction on abdominal aortic aneurysm surfaces”. Artificial Intelligence in Medicine, 103412. https://doi.org/10.1016/j.artmed.2026.103412
Recommended Hashtags
#ArtificialIntelligence #MedicalAI #AneurysmResearch #PrecisionMedicine #VascularHealth #DeepLearning #ScienceCommunication #Medmultilingua
© Medmultilingua 2026 — Science accessible to everyone, worldwide.
Leave a Reply